
.jpeg)
Case Series/Study
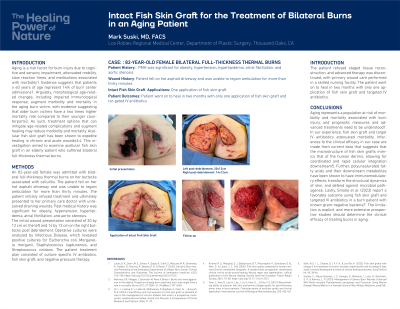
An 82-year-old female was admitted with bilateral full-thickness thermal burns on her buttocks associated with cellulitis. The patient fell on hot asphalt driveway and was unable to regain ambulation for more than thirty minutes. The patient initially refused treatment and ultimately presented to her primary care doctor with unresolved draining wounds. Past medical history was significant for obesity, hypertension, hyperlipidemia, atrial fibrillation, and aortic stenosis.
The initial wound presentation consisted of 20 by 12 cm on the left and 14 by 12 cm on the right buttocks post debridement. Operative cultures were analyzed by Infectious Disease, which revealed positive cultures for Escherichia coli, Morganella morganii, Staphylococcus lugdunensis, and Streptococcus viridans. The patient treatment plan consisted of culture specific IV antibiotics, fish skin graft, and negative pressure therapy.
Results:
The patient refused staged tissue reconstruction, and advanced therapy was discontinued, with primary wound care performed in a skilled nursing facility. The patient went on to heal in two months with only one application of fish skin graft and targeted IV antibiotics.
Discussion:
Aging represents a population at risk of morbidity and mortality associated with burn injury, and prognostic measures and advanced treatments need to be understood1. Inferences to the clinical efficacy in our case are made from current data that suggests that the microstructure of fish skin grafts mimics that of the human dermis, allowing for coordinated and rapid cellular integration downstream5. Further, polyunsaturated fatty acids and their downstream metabolites have been shown to have immunomodulatory effects. Lastly, Smolle et al. (2023) report a favorable outcome using fish skin graft and targeted IV antibiotics in a burn patient with known gram-negative bacteria7. The limitation is explicit, and more extensive prospective studies should determine the clinical efficacy of treating burns in aging.