
.jpeg)
Clinical Research
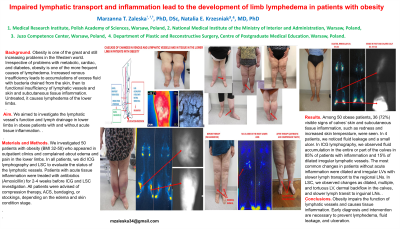
Obesity is one of the significant and still increasing problems in the Western world. Irrespective of problems with metabolic, cardiac diseases, and diabetes, obesity is one of the more frequent causes of lymphedema. Increased venous insufficiency leads to accumulations of excess fluid with bacteria drained from the skin, then leads to functional insufficiency of lymphatic vessels and skin and subcutaneous tissue inflammation. Untreated causes lymphedema of lower limbs.
We aimed to investigate the lymphatic vessel’s function and lymph drainage in lower limbs in obese patients with and without acute tissue inflammation.
Methods:
We investigated 50 patients with obesity (BMI 32-50) appearing in the outpatient clinic and complaining about edema and pain in the lower limbs. In all patients, we did ICG lymphography and LSC to evaluate the lymphatic vessel status. Patients with acute tissue inflammation were treated with antibiotics (Amoxicillin) for 2-4 weeks before ICG and LSC investigation. All patients were advised compression therapy, ACS, bandaging, or stockings, depending on the edema stage and skin condition.
Results:
Among 50 obese patients, in 36 (72%), visible signs of calves’ skin and subcutaneous tissue, such as redness and increased skin temperature, were seen. In 4 patients, we noticed fluid leakage and a small ulcer. In ICG lymphography, we observed fluid accumulation in the entire or part of the calves in 85% of patients with inflammation and in 15% of dilated irregular lymphatic vessels. The most common changes in patients without acute inflammation were dilated and irregular LVs with slower lymph transport to the regional LNs. In LSC, we observed enlarged, multiple, and tortuous LV changes, dermal backflow in the calves, and slower lymph transit to inguinal LNs.
Discussion:
Conclusion. Obesity impairs lymphatic vessel’s function and causes tissue inflammation. Early diagnosis and intervention are necessary to prevent lymphedema development, fluid leakage, and ulceration.