(WHS-P76) Wound Care in End-Stage Dermatomyositis: A Case Report
Friday, May 17, 2024
7:30 AM - 5:00 PM East Coast USA Time
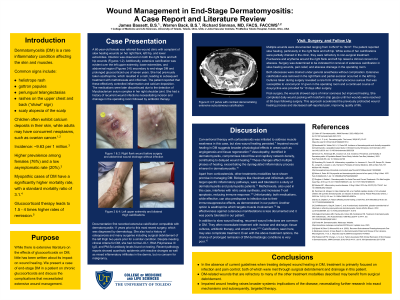
Background Dermatomyositis (DM) is a rare inflammatory condition of the skin and muscle with a variety of clinical findings including characteristic skin presentations, calcium deposits, and concommitant cancer diagnoses. We share the case of a patient utilizing glucocorticoid treatment for end-stage DM and discuss the influence of disease and treatment that complicate wound management. Case Presentation A 60-year-old female presented to the wound clinic for slow healing hip and lower extremity wounds with signs of infection on both hip wounds despite negative cultures. She also exhibited extensive extremity and abdominal calcifications secondary to end-stage dermatomyositis and chronic daily glucocorticoid use of 7 years. She has a history of other immunosuppressive medications such as azathioprine, methotrexate, and infliximab injections in addition to history of previous sugrical debridement. Despite meeting clinical criteria for DM, she had normal JO-1, RNA Polymerase III IgG, and PM-Scl antibody levels found on testing. Multiple wounds were documented, with terribly slow healing courses, calcium deposits were drained in clinic, and finallly surgical debridement was successful. Discussion Dermatomyositis presents numerous challenges in management, particularly in advanced stages of the disease. This case highlights a notable manifestation of slow wound healing, emphasizing the complexities involved in the treatment approach. Evidence of vasculopathy in DM has been integral to this process leading to compromised blood flow. More specifically, DM patients often have decreased capillary network density. Changes on these fronts affect the proliferation and remodeling phases of healing in addition to the inflammatory process that is inherently dysregulated in DM. In managing this end-stage dermatomyositis case, conventional therapeutic approaches involving corticosteroids were implemented and continue to be utilized with this patient today, the current standard of care. Bologics such as monoclonal antibodies (rituximab, infliximab) also used have shown to be well tolerated in paatients with dermatomyositis and polymyositis. Methotrexate, has also shown some efficacy. Azathioprine well targets the muscle involvement of DM, but there is limited literature suggesting efficacy addressing the cutaneous aspects of the disease. Conclusion In summary, this case report highlights the intricate challenges associated with managing end-stage dermatomyositis, notably emphasizing the complication of slow wound healing. Despite the efficacy of conventional treatments such as corticosteroids and adjunctive therapies like biologics and methotrexate, the persistent issue of impaired wound healing raises broader systemic implications of the disease. A deeper understanding of the intricate vascular mechanisms could elucidate more targeted interventions.

.jpeg)