(WHS-P29) The Impact of Topical Oxygen Therapy on Wound Healing: Assessing Efficacy and the Influence of Patient Characteristics in a Single-Institution Retrospective Chart Review
Friday, May 17, 2024
7:30 AM - 5:00 PM East Coast USA Time
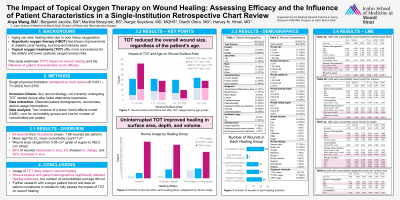
Background: Aging can diminish wound healing due to insufficient tissue oxygenation. Hyperbaric oxygen therapy (HBOT) poses systemic risks, while topical oxygen treatments (TOT) offer a safer localized alternative. This study examines TOT's impact on wound healing and how patient and wound characteristics influence its effectiveness.
Methods: A retrospective chart review (8/1/2011 - 7/1/2023) analyzed patients aged 23 to 97 with any wound etiology who used TOT (GWR Medical inc.) after unsuccessful alternate treatments. The device was used 90 minutes daily for four days, followed by a three-day break. Patient demographics (gender, age, race, smoking status, comorbities, radiation usage, nutrition level), wound details (dimensions, age, location, etiology), and device usage interruptions were collected from EPIC. Comorbidities were subdivided into body-system categories. Wound dimensions were measured using a centimeter ruler. Healing was gauged by percent changes in surface area, depth, and volume between the initial and final measurements. Analysis included two linear mixed effects (LME) models—one for comorbidity groups and one for individual comorbidity counts. Variables with high collinearity and variance inflation factor (VIF) > 10 were removed.
Results: From 45 patients, 84 wounds were reviewed, averaging 1.86 wounds and 7.27 comorbidities per individual. Wound sizes ranged from 0.08 cm2 to 482.5 cm2 (median: 10.25 cm2). About 68% of wounds shrank, 2% remained unchanged, and 30% enlarged. Complete healing was more prevalent in nourished patients (94%), those without radiation history (88%), and non/former smokers (53%, 41%). No wound exceeding 27 cm2 completely healed. The LME model with comorbidity count showed the percent of days used enhanced healing for surface area (β = 1.092, p = 0.017), depth (β = 0.954, p = 0.030), and volume (β = 1.021, p = 0.027). Certain locations (foot: β = 1.597, p = 0.022; leg: β = 1.259, p = 0.027; toe: β = 2.498, p = 0.003) and being male (β = 1.537, p = 0.012) promoted healing. Initial depth (β = -0.472, p = 0.018) and white ethnicity (β = -2.033, p = 0.013) reduced healing. Overall comorbidity count was insignificant (β = 0.093, p = 0.422). The LME model with comorbidity categories found that being male (β = 1.486, p =0.019), percent of days used (β = 1.002, p = 0.032), and bone disease (β = 2.327, p = 0.008) increased surface area healing, while initial depth remained detrimental (β = -0.519, p = 0.007). Age was a non-factor in both models.
Conclusion: Uninterrupted TOT usage promoted surface area, depth, and volume healing, while greater initial depth hindered healing. Given that certain wound and patient characteristics can influence healing with TOT, physicians should consider these factors when tailoring patient treatment plans.

.jpeg)