(WHS-P24) Effect of pre-operative wound characteristics and previous treatments on pressure ulcer healing outcomes and disposition
Friday, May 17, 2024
7:30 AM - 5:00 PM East Coast USA Time
Background: Pressure ulcers are injuries to the skin and underlying tissue that often develop into chronic wounds and can significantly impact quality of life. After surgical closure, many patients experience complications such as dehiscence, maceration, drainage, and necrosis, and may require long-term rehabilitation to achieve functional recovery. The objective of this study is to evaluate the association between wound characteristics prior to surgical closure and wound healing outcomes including complication rates and disposition.
Methods: In this prospective study, patients with grade III/IV buttock pressure ulcers were admitted for surgical closure and observed post-operatively for at least 14 days. Wound characteristics upon admission, such as wound location, size of wound (length, width, depth), and previous wound treatment (previous closure, debridement, negative pressure wound therapy, hyperbaric oxygen, biologics, revascularization) were recorded. Wound volume was estimated by multiplying length, width and depth. Outcome measures included 2-week complication rates, length of hospital stay, disposition, and wound closure rates at 2 weeks, 1 month, 6 months, and 12 months. Odds ratios and t-tests were used to analyze outcomes.
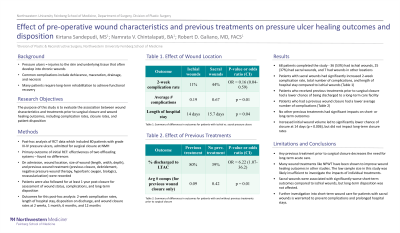
Results: Of a total of 68 patients who completed the study, 36 (53%) had ischial wounds, 25 (37%) had sacral wounds, and 7 had wounds in other locations. 11% of patients with ischial wounds experienced complications, while 44% of those with sacral wounds experienced complications (OR=0.16, 95% CI 0.04-0.59). The average number of complications per patient was 0.19 in patients with ischial wounds and 0.67 in patients with sacral wounds (p = 0.01). Patients with sacral wounds also had a longer average hospital stay than those with ischial wounds, by 1.7 days (p = 0.04). Increased wound volume was associated with lower chance of closure at 14 days (p = 0.006), but did not have an effect on closure rates at long-term follow-ups. Increased wound length was also independently associated with lower chance of closure on day 14, although this result only approached significance (p = 0.056). Patients who did not receive any previous treatments were more likely to be discharged to a long-term care facility than patients who had previous treatment (OR=6.22, 95% CI 1.07-36.2). The average number of complications per patient was 0.09 for patients who had previous wound closure and 0.42 for patients who had not had previous closure (p = 0.01).
Conclusion: Overall, this study found that wound characteristics prior to surgical closure, including size, location, and previous treatments, have a significant impact on post-operative complication rates and disposition in patients with grade III/IV buttock pressure ulcers. These findings warrant further investigation and can help guide management and pre-operative counseling.

.jpeg)