(PI-035) Successful Healing of Complex Lower Limb Amputation Wounds with A Novel Transforming Powder Dressing (TPD)
Thursday, May 16, 2024
7:30 PM - 8:30 PM East Coast USA Time
Introduction: In the United States, approximately 150,000 people undergo below knee amputations (BKA) annually largely due to diabetes, peripheral vascular disease, and trauma.1 Wound healing complications such as infection, tissue necrosis, and dehiscence, on BKA sites pose special challenges because these wounds may prevent or delay ambulation with a prosthetic limb2,3. Surgical wound management paradigms have moved into a new era, and correct choice of wound dressing is paramount to achieve the appropriate moisture balance within the wound.3,4 We review a complex case in which current standard of care (SOC) treatment failed and transforming powder dressing (TPD) was successfully used to facilitate wound healing.
Methods: A 32-year-old male ballroom dance instructor who developed sudden onset of vertigo was admitted to the hospital with shock, fulminant community acquired bacterial meningitis, disseminated intravascular coagulation (DIC), and purpura fulminans (an extreme thrombotic subtype of DIC). Hospital course was c/b acute renal and respiratory failure, extensive skin necrosis, and gangrene resulting in bilateral BKAs.
Post-surgical BKA wound management was challenging due to the significant amount of exposed soft tissue that was unable to be surgically closed. Treatment with negative pressure wound therapy (NPWT) was initiated. Due to NPWT related pain and thrice weekly dressing changes, the patient complained of consistent pain (8/10). To address pain management, wound care was modified and NPWT was discontinued. Treatment of the extensive wounds was converted to TPD, a commercially available powder dressing that forms a moist, oxygen-permeable barrier that covers and protects the wound.
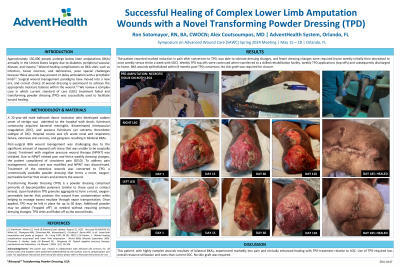
Results: The patient reported marked reduction in pain after conversion to TPD, was able to tolerate dressing changes, and fewer dressing changes were required (twice weekly initially then decreased to once weekly). When transferred to a skilled rehabilitation facility, weekly TPD applications were continued, and continued when discharged to home. BKA wounds epithelialized within 8 months post-TPD conversion. No skin graft was required for closure.
Discussion: This patient, with highly complex wounds resultant of bilateral BKAs, experienced markedly less pain and clinically enhanced healing with TPD treatment relative to SOC. Use of TPD required less overall resource utilization and costs than current SOC. No skin graft was required.

.jpeg)