
.jpeg)
Evidence-Based Practice
Even a perfectly debrided wound may have difficulty healing if the topography of the wound base or edges is unfavorable. A wound with an elevated base relative to the periwound will have impaired keratinocyte migration and stalled healing. If wound edges are vertical, display epiboly, or undermined areas, the wound will also have difficulty healing. Wound remodeling may need to be performed in such cases.
Methods:
Wound remodeling typically involves lowering the wound base and resecting wound edges at a 45-degree angle. While adjusting the wound base is usually straightforward, edge modifications can be complicated. “Edge trenching, “soap scrap,” and “parallel pocket incision” techniques were developed to facilitate closure of wounds where edge resection is not possible or desired.
Results:
The topography of the ideal wound includes a base that is at the periwound level or slightly lower and edges resembling a shallow plate (at 45 degrees or less angle to the wound bed). We will review four typical scenarios when wound remodeling is usually needed and the techniques that can be used in each case.
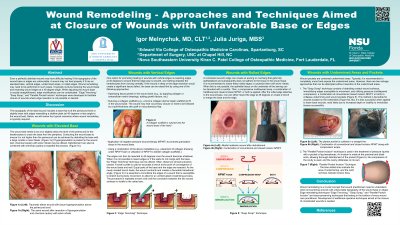
1.) Wounds with raised base.
2.) Wound with vertical edges.
3.) Wounds with rolled edges.
4.) Wounds with undermined areas and pockets.
Discussion:
Wound remodeling is a crucial concept that wound practitioners need to understand when encountering wounds with unfavorable topography of the wound base or edges. Edge remodeling techniques “Edge trenching,” “Soap Scrap,” and “Parallel Pocket Incision” are tissue-preserving techniques that belong in the toolbox of every wound care practitioner. Development of additional operative techniques aimed at closure of complicated wounds is needed.