
.jpeg)
Case Series/Study
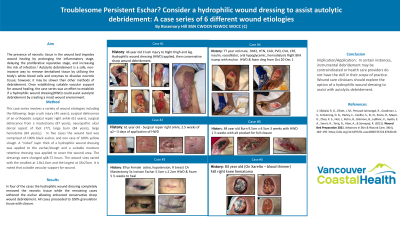
This case series involves a variety of wound etiologies including the following: large crush injury (45 years), surgical dehiscence of an orthopedic surgical repair right ankle (61 years), large burn (84 years), surgical dehiscence from a mastectomy (87 years), large hematoma (84 years), neuropathic ulcer dorsal aspect of foot (77). In five cases the wound bed was comprised of 100% black eschar, and one case of 100% yellow slough. A “nickel” layer thick of a hydrophilic wound dressing was applied to the eschar/slough and a suitable moisture retentive dressing was applied to cover the wound area. The dressings were changed q48-72 hours. The wound sizes varied with the smallest at 1.8x1.6cm and the largest at 33x23cm. It is noted that suitable vascular support for wound healing was established prior to proceeding with autolytic debridement.
Results: In four of the cases the hydrophilic wound dressing completely removed the necrotic tissue while the remaining cases softened the eschar allowing enhanced conservative sharp wound debridement. All cases proceeded to 100% granulation tissue with closure.
Discussion:
In certain instances, instrumental debridement may be contraindicated or health care providers do not have the skill in their scope of practice. Wound care clinicians should explore the option of a hydrophilic wound dressing to assist with autolytic debridement.