
.jpeg)
Clinical Research
We evaluated arterial anatomic aberrancies seen in the areas with described terminal skin lesions and applied Hagen-Poiseuille's flow rate law to the alteration of perfusion leading to ischemic skin changes at the time of hypotension.
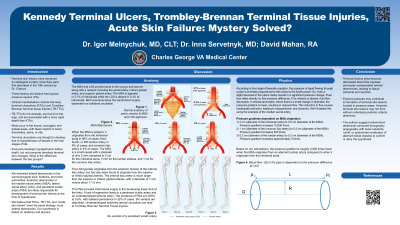
Results: Median sacral artery (MSA) and lateral sacral arteries (LSAs) provide blood supply to sacrum and coccyx. These arteries are embryologically absent in 2.4% of individuals in which case the blood supply in the affected areas depends on the collateral blood vessels. The collaterals have smaller diameters than the originally intended arteries.
When MSA is present, it originates from the aorta in 90% of cases. However, when it comes off lumbar arteries (6% of cases), and the common iliac artery (4% of cases), the afferent vessels have smaller diameters. Subsequently, the diameter of the afferent vessels drops from about 2 cm (aorta) to 0.3 cm (lumbar arteries), and this leads to a significant changes of flow gradient at the time of hypotension causing hypoperfusion.
Terminal skin injuries of lower extremities may be due to persistent sciatic artery (PSA) seen in 0.6% of individuals. Sciatic artery normally regresses by the 3rd month of embryonic development. If it does not regress, PSA leads to underdeveloped femoral arterial system susceptible to hypotensive insults and subsequent ischemia causing characteristic terminal skin lesions.
Discussion:
Anatomic arterial aberrancies of the pelvic or lower extremity vessels are likely responsible for terminal skin lesions. Local arterial aberrancies may also mimic or contribute to pressure injuries resulting from significant hypotension among individuals who survive hypotensive episodes and may be an unrecognized critically important risk factor for pressure injury formation. Antemortem angiography or postmortem evaluation of aberrant blood vessels are needed to confirm or dispute this hypothesis and we request the wound care community for assistance.