Introduction: In the US it is estimated that, annually, 500,000–600,000 people have a venous leg ulcer (VLU), at an estimated cost of $3.5 billion USD,1 accounting for approximately 2% of total annual US healthcare costs.2 In 2019, Medicare expenditure alone for VLU as a principal diagnosis was >$1.1 billion USD.3 An analysis of Medicare patients with a VLU, including infection costs, was $1.2 billion USD in 2014 at the higher-end estimate.4 Previous studies suggest that about 60% of VLUs will heal within 12 weeks, with recurrence rates ranging from 30% at one year to 78% by two years.5The objective of this study was to retrospectively evaluate the comorbidities, treatment patterns and outcomes of Medicare enrollees who developed VLUs.
Methods: Medicare Limited Data Standard Analytic Hospital Inpatient and Outpatient Department Files were used to follow patient episodes who received medical care for a VLU from October 1, 2015 through October 2, 2019. Patients diagnosed with chronic venous insufficiency and a VLU were propensity matched into four groups based on their treatment regimen. Episode claims were used to document demographics, comorbidities, and treatments of Medicare enrollees who develop VLUs and important outcomes such as time to ulcer closure, rates of complications, and hospital utilization rates. Outcomes were compared across key propensity matched groups.
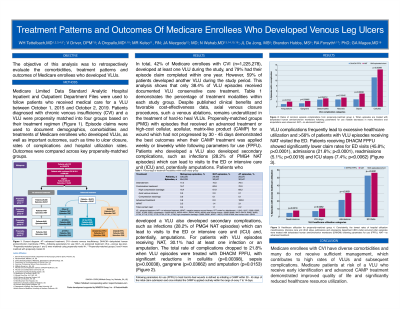
Results: Forty-two percent of Medicare enrollees with chronic venous insufficiency (1,225,278), developed at least one VLU during the study, and 79% had their episode claim complete within one year. However, 59% of patients developed another VLU during the study period. This analysis shows that only 38.4% of VLU episodes received documented VLU conservative care treatment. Propensity matched episodes which received an advanced treatment or high-cost cellular, acellular, matrix-like products (CAMPS) for a wound which had not progressed by 30 days saw the best outcomes when their treatment was applied weekly or biweekly (following parameters for use) (Figure 1). Complications such as rates of infection (33%), and emergency department visits ( >50%) decreased among patients who received a CAMP while following parameters for use (Figure 2).
Discussion: Medicare enrollees with chronic venous insufficiency have diverse comorbidities and many of these patients do not receive sufficient management which contributes to high rates of VLUs and subsequent complications. Medicare patients at risk for a VLU who receive early identification and advanced treatment demonstrated improved quality of life and significantly reduced healthcare resource utilization.

.jpeg)